
What Radiography Types Are Used?
There are many types of radiography used to assess structural deficits in velopharyngeal disorders. While Multi-View Videofluoroscopy is the most common clinical technology, many others have been documented in the research literature. This section will briefly describe:
-
Multi-View Videofluoroscopy (MVF)
-
Magnetic Resonance Imaging (MRI)
-
Computed Tomography (CT) Scan
-
Cephalography
Multi-View Videofluoroscopy
Multi-view videofluoroscopy allows a 2-dimensional view of velum movement but reduces radiation exposure by using pulsed fluoroscopy. This technique can be used for surgical planning for VPI correction. This imaging technique may be useful in otherwise uncooperative or agitated patients who will not allow nasendoscopy. It is the same radiographic technology used to perform a modified barium swallow to assess dysphagia.
Source: Berger, M.K.. (2011) Instrumental Assessment of Velopharyngeal Dysfunction: Multi-view Videofluoroscopy vs. Nasopharyngoscopy [pdf].http://www.ohioslha.org/pdf/Convention/2011%20Handouts/SC18Voice BergerL.pdf
Magnetic Resonance Imaging
MRI is used to evaluate the velopharyngeal mechanism and can allow a 3-dimensional image using a heavy electromagnetic field (see images below). While it requires patient cooperation, it is the least invasive of direct VPI assessment. This imagining technology allows for dynamic evaluation of muscular morphology and eliminates exposure to radiation. However, this MRI cannot be used in non-compliant patients (e.g., will not lie still) or in patients with any type of in-dwelling metal prostheses (e.g., metal hip replacement).


Computed Tomograhy Scan
CT Scans will allow for both 3- and 4-dimensional views of velopharyngeal structures, however the images are static (see image below). While the images are less clear than some high-tesla MRI scans, the examination duration is shorter than MRI. The disadvantages of this technology include the amount of radiation exposure during the imaging process. This process is largely used in research applications.
Source: Honjo, I., Mitoma, T., Ushiro, K., & Kawano, M.. (1984) Evaluation of Velopharyngeal Closure by CT Scan and Endoscopy. Plastic Reconstruction and Surgery. 74(5): 620-625.

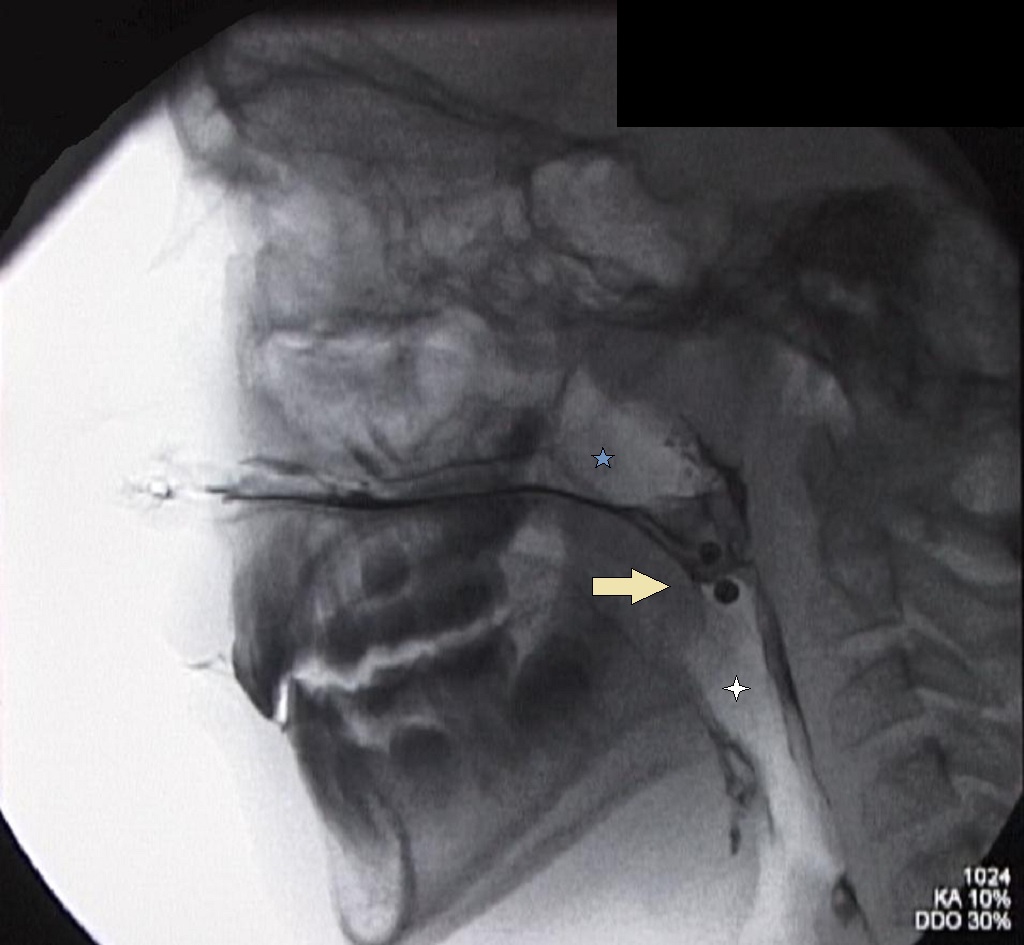
Cephalography
Cephalograms were one of the first x-ray technologies used to visualize the velopharyngeal structures (i.e., nasopharynx and velum). Due to the high amount of radiation delivered, difficulty in interpretation, and lack of visualization of the velum movements during speech, the procedure is rarely used today (see image below).
Source: Sakamoto, Y., Shigeyoshi, S., Jinzaki, M., Yamada, Y., Ogata, H., & Kishi, K.. (2015). Evaluation of Velopharyngeal Closure by 4D imaging using 320-detector-row computed tomography. Journal of Plastic, Reconstructive, & Aesthetic Surgery. 68(4): 479-484.

Recommended Readings
Atik, B., Bekerecioglu, M., Tan, O., Etlik, O., Davran, R., & Arslan, H. (2008). Evaluation of dynamic magnetic resonance imaging in assessing velopharyngeal insufficiency during phonation. Journal of Craniofacial Surgery,19(3), 566-572.
Bae, Y., Kuehn, D. P., Sutton, B. P., Conway, C. A., & Perry, J. L. (2011). Three-dimensional magnetic resonance imaging of velopharyngeal structures.Journal of Speech, Language, and Hearing Research, 54(6), 1538-1545.
Lipira, A. B., Grames, L. M., Molter, D., Govier, D., Kane, A. A., & Woo, A. S. (2011). Videofluoroscopic and nasendoscopic correlates of speech in velopharyngeal dysfunction. The Cleft Palate-Craniofacial Journal, 48(5), 550-560..
Shprintzen, R. J., & Marrinan, E. (2009). Velopharyngeal insufficiency: diagnosis and management. Current Opinion in Otolaryngology & Head and Neck Surgery, 17(4), 302.
Tian, W., Yin, H., Redett, R. J., Shi, B., Shi, J., Zhang, R., & Zheng, Q. (2010). Magnetic resonance imaging assessment of the velopharyngeal mechanism at rest and during speech in Chinese adults and children. Journal of Speech, Language, and Hearing Research, 53(6), 1595-1615.